Ankylosing Spondylitis treatment in Pune
Ankylosing Spondylitis: Symptoms, Diagnosis, and Treatment
Ankylosing spondylitis is a chronic inflammatory rheumatic disease that primarily affects the axial skeleton, including the sacroiliac joints and spine. However, it can also impact peripheral joints, enthesis, eyes, and, in rare cases, the heart and lungs.
Understanding Ankylosing Spondylitis
The term “ankylosis” refers to fusion, “spondy” relates to vertebrae, and “itis” indicates inflammation. In short, “ankylosing spondylitis” is an inflammatory condition of the spine that, if left untreated, can lead to the fusion of vertebrae.
This type of arthritis, which affects the joints of the spine and sometimes peripheral joints, falls under the category of spondyloarthropathies.
Types of Spondyloarthropathies
The spondyloarthropathy family includes:
- Ankylosing spondylitis
- Psoriatic arthritis (arthritis linked with psoriasis)
- Reactive arthritis
- Spondyloarthritis associated with Crohn’s disease or ulcerative colitis
Juvenile-onset spondyloarthritis
These conditions are also known as seronegative spondyloarthropathies, meaning they are negative for rheumatoid factor. Ankylosing spondylitis commonly affects young adults between 18 and 30 years and is more prevalent in males (3:1 ratio).
Genetic Component: HLA-B27
The HLA-B27 gene is strongly associated with ankylosing spondylitis. However, it’s important to note:
- Being HLA-B27 positive does not guarantee the disease. Up to 8% of the normal population carries this gene, but only 1-6% of them develop spondyloarthropathy.
- Being HLA-B27 negative does not rule out the disease. Diagnosis is based on clinical symptoms, such as inflammatory low back pain, buttock pain, uveitis, and tendinitis.
Common symptoms :
- Sudden onset of low back pain or pain in the buttock region, often shifting sides
- Morning stiffness or pain after long periods of inactivity
- Peripheral joint arthritis, mainly affecting lower limb joints
- Heel pain or history of persistent heel pain
- Dactylitis, which is painful inflammation of fingers or toes
- Low-grade fever, fatigue, weakness, and weight loss
- Eye involvement, leading to pain, redness, and blurry vision
- Intestinal inflammation, increasing the risk of Crohn’s disease or ulcerative colitis
- Fusion of vertebrae, causing a stiff spine and stooped posture
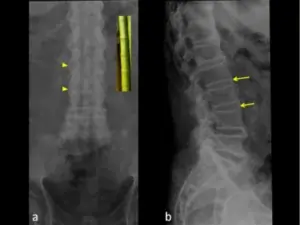
Diagnosis of Ankylosing Spondylitis:
Diagnosis is based on a combination of:
- Clinical signs and symptoms
- X-rays and MRI findings
- Blood tests (HLA-B27 and inflammatory markers)
Ankylosing Spondylitis Treatment in Pune
The goal of treatment is to manage symptoms, slow disease progression, and maintain mobility.
1. NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
NSAIDs are first-line treatment and help relieve pain and stiffness. Studies show that long-term NSAID use may slow disease progression. However, long-term use requires monitoring due to potential stomach ulcers and kidney issues.
2. DMARDs (Disease-Modifying Anti-Rheumatic Drugs)
- Sulfasalazine: Effective for axial disease.
- Methotrexate: Useful for peripheral arthritis.
3. Biologic Therapies (Anti-TNF Agents)
For severe cases unresponsive to NSAIDs and DMARDs, biologics like Adalimumab, Etanercept, and Infliximab can be prescribed. These drugs reduce pain, stiffness, and inflammation but may increase infection risk.
4. Physiotherapy and Exercise
- Helps maintain mobility and reduce stiffness
- Includes stretching, strengthening, and posture correction exercises
5. Adjunctive Treatments
- Bisphosphonates, calcium, and vitamin D for bone health
- Corrective surgery if necessary
Conclusion
Ankylosing spondylitis is a chronic condition requiring early diagnosis and management. If you or someone you know is experiencing symptoms, consult a specialist for Ankylosing Spondylitis treatment in Pune to receive a personalized treatment plan and prevent disease progression.